Can the Chemistry (pH) of the Blood and Interstitial Fluids of the Interstitium be Altered?
Can the Chemistry Including the pH of the Blood and Interstitial Fluids of the Interstitium be Altered by YOUR Lifestyle and Dietary Choices?
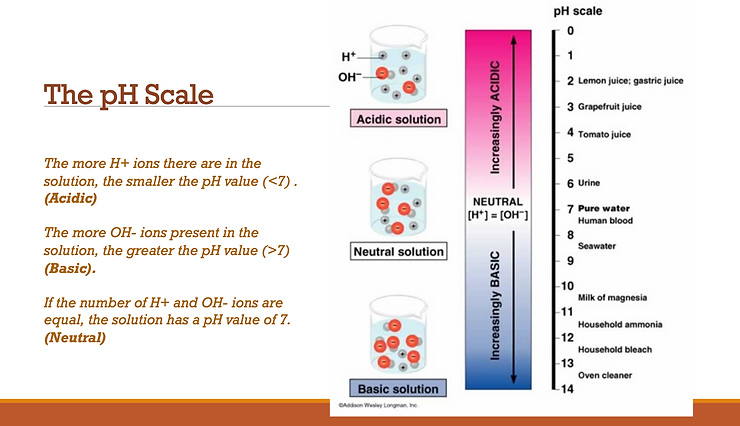
The alkalinity of the blood above pH 7.365 (alkaline phosphate)—any rise—is a result or a compensatory reaction due to over-acidity in the interstitial fluids of the Interstitium as the blood attempts to maintain pH balance at 7.365. There is no exception for this rule of alkalinity. The body will ALWAYS overcompensate for the excess acidity in the interstitial fluids of the Interstitium by over-alkalizing the blood to maintain homeostasis. I call this the “teeter-totter” effect. Along comes the conventional medical attendant and perceives that there is too much alkalinity, when really there is not.[1]
This is an important concept to grasp, so let’s oversimplify a bit. The interstitial fluids of the Interstitium have become acidic. The blood “knows” that. So, it pours out extra alkalinity or alkaline phosphate into the blood and the blood pH spikes up to a higher than normal pH. It’s like when we get the bejeebers scared out of us by something innocent, we over-react. When suddenly alarmed, a person might scream, holler, faint, get mad, strike out, drop the vase, kick the dog, or even have a heart attack. The blood does the same thing. A knee-jerk reaction…well, actually, a blood-jerk reaction.

Alternatively, how many times have you heard of a car going off the shoulder of the road and the driver over-reacts, jerks the wheel back, and flies into the other lane of oncoming traffic. It happens all the time. Incidentally, if that does happen to you, you’re better off not to interfere. Stay on the shoulder. Let the wheel stay there for a moment. Slow the car down. But don’t overreact.
Mainstream medicine, not understanding the cause of the excessive alkalinity pouring into the body, may try to stop the rushing over-alkalization. But that’s the wrong move. We’re better off not to interfere.
Once more. When your little boy falls down, sees mama going out the door, or is scared of the boogey man, what happens? He not only cries, but how often do we see a child go into a big, fat over-reaction? Sometimes, they really get worked up. It’s a natural over-reaction to a typical situation.
Now it’s Dad’s turn to over-react. Along comes Dad and says to keep quiet, shut-up, don’t be such a little sissy, put a lid on it, grow up, stop that crying, OR ELSE…
Since I have digressed to make a point, I may as well digress all the way. Wrong move, Dad. If you do that often enough, the message you send to your child is don’t have feelings, don’t express your feelings, you are not acceptable, don’t act like a child even though you are a child, and don’t be who you are. So don’t over-react Dad. Better to let the child get it out, stay in the room, validate their feelings, and use a little Active Listening (www.gordontraining.com). Strong feelings can come and go…or come and stay. If you’re really klutzy, you could be orchestrating chronic emotional issues for a lifetime. Gee, thanks Dad.
Now, back to your blood. Interstitial fluids that surround every cell in the body are acidic. Here comes a flood of alkalinity—even so much that the pH rises and concerns the western medical establishment. But whatever it was that caused the pH to over-react must be understood. Acidic interstitial fluids of the Interstitium mean problems ahead, correct? Not only do we need alkalinity but lots of it. The acidic interstitial fluids that surround the cells will soon even out the rise in blood pH, and we will need additional alkalinity to wipe out the acidic interstitial fluid problem.
Liver cancer is not a disease of alkalinity but a disease of acidity. The body uses the calcium of the bones as well as other buffers (bicarbonate, hemoglobin, sodium, etc.) to chelate or neutralize acidity! That is why there are always microcalcifications in the liver before the liver cancer or tumor shows up. Why prior to the tumor? Because the body will always try to protect and preserve itself by buffering acids with the alkalinity of calcium. The bones are always affected in any cancer because the bones are an excellent source for calcium. So is liver cancer the disease? No.
Then is the loss of bone mass the disease or the calcium deposits in the liver the disease. NO?
Is the increase in the alkaline phosphates the disease? NO! NO!
These are all symptoms, not diseases!
Then the disease must be the over-acidity? Well yes, and well no.
Then what is the disease? The “yes” part I call acidosis or hyperacidity. That is an acceptable term for the condition. But it is really much more. The “no” part is that it’s more than acidity. It’s a psychological disorder. It’s a sociological malaise. It’s a cultural-anthropological phenomenon. And once people understand the truth and the scientific foundation of the New Biology, and once people understand the science of what I have been writing about for three the better part of three decades, it may than become to be understood as a “moral disease” as well.
And why is that, you ask? Is committing suicide a moral issue? Well, yes. Is drinking yourself to death a moral issue? Well, yes. Is allowing your children to become obese flying in the face of natural law? Well, yes, assuming you are aware of what’s happening and have other options.
If you say “yes” to these last few questions, then we are looking at a very, complex psychological, sociological, cultural, biological and moral phenomenon. Once you know and believe that over-acidity causes every disease and most dis-ease, then to ignore that fact is a form of suicide. When you eat poorly, you pull the trigger every day of your life, and eventually, the gun fires. The bullet might hit you square in the head like a massive heart attack, or it may kill you more slowly like a cancer, or it may simply put you in a fog for the next 15 years like Alzheimer’s or dementia.
This “disease-phenomenon” is an inverted way of living, eating, breathing and thinking!!! Yes, this is the cause of ALL disease—ALL that disturbs the central balance of organized matter that leads to excess acidity in the fluids of the body. It is ALL that leads to increases in alkaline phosphates. It is ALL micro-calcifications in the liver, ALL liver tumors, ALL liver cancer and ALL potential bone cancer!!!!
First, we must understand that ALL of the above sicknesses and diseases are NOT sicknesses or diseases but a symptom of systemic acidosis and catarrh that has built up in the blood and then interstitial fluids that has significantly effected the white blood cells’ ability (the janitorial and garbage collectors for the blood and tissues) to remove metabolic acids and morbid matter. When we are dealing with any symptom or any effect, we need to look to the cause. To understand the cause is not difficult nor is the understanding of the treatment.
The “New Biology” explains the cause and effect of all sickness and disease in addition to explaining how to improve the quality and quantity of life. For example, enervation (the deprivation of force or strength) and muscle weakness per se is not a disease. Weakness, or lost power, is not a disease; but, by causing a flagging of the elimination of tissue-waste which is toxic, the blood and then interstitial fluids become charged with acids.
I refer to this as systemic acidosis—poison in the blood and interstitial fluids that surround all body cells. This is disease and when the toxin accumulates beyond the toleration point, a crisis takes place. This means that the poison or acid is being eliminated—often through the skin, the third kidney. We can call this disease, but it is not. The only disease is systemic acidosis which localizes in the compartments of the Intersititum and effects the weakest parts of our body.

And what we call disease is symptoms produced by the forced vicarious elimination of acids through the mucous membranes. When the elimination takes place through the mucous membranes of the nose, it is called a cold—catarrh of the nose. And where these crises are repeated for years, the mucous membranes thicken and ulcerates, and the bones enlarge, closing the passages. At this stage, hay fever or asthma develops. When the throat and tonsils, or any of the respiratory passages, become the seat of the crises of acidity, we have croup, tonsillitis, pharyngitis, laryngitis, bronchitis, asthma, pneumonia, etc.
When the acids locate in the cranial cavity we have dementia, Parkinson’s, Alzheimer’s, muddle thinking, forgetfulness, and even depression. When the acids locate in the gastrointestinal tract we have IBS, gastrointestinal dysmotility, autonomic dysfunction, carotid stenosis and ischemic colitis. When the acids are expressed through the skin we have psoriasis and melanoma cancer. When the acids locate in the liver tissue we have micro-calcifications of these acids that lead to tumors and liver cancer.
What’s in the name?
All are symptoms of the expulsion of acids from the blood and the interstitial fluids that surround the tissues, organs and glands at the different points named. They are of the same character essentially and evolve from the one cause, namely, systemic acidosis, a crisis of toxemia. [2]

The description can be extended to every organ of the body, including the second largest organ, the skin (the Interstitium is the largest organ of the body). For any organ that is enervated below the average standard from stress of habit, from work, or worry, from injury, or any other cause, that organ may become the location of the crises of systemic acidosis. The symptoms presented differ with each organ affected. That fact gives color to the erroneous belief that every symptom-complex is a separate and distinct disease. But, thanks to the new light being shed by the “New Biology” upon nomenclature involved in the naming of a disease, every symptom-complex goes back to the one and only cause of all diseases, namely, systemic acidosis of the interstitial fluids of the Interstitium.[1]
To find the cause of all symptomologies including liver, pancreatic, bowels, prostate, lung, breast or bone cancer, start with colds and catarrh, and watch the pathology as it travels through the seven stages of acidity, from sensitivity, irritation (IBS), catarrh, inflammation, induration (lupus), ulceration and then to degeneration—cancer. How well could you try to find the cause of man by ignoring his conception, embryonic life, childhood, manhood, etc. Nature’s order is interfered with by enervation habits until systemic acidosis is established. Then a vaccination (seen in Gulf War Syndrome and Spanish Flu Epidemic) or an infection (actually an outfection) from any source will act as a firebrand. Sooner or later cause the most vulnerable organ (the bowels) will undergo organic change. The organ, however, has nothing to do with cause, and directing treatment toward the organ compounds the problem and is nonsense. Examples of this wrong thinking yields blood transfusions for pernicious anemia, gland hormonal treatment for gland impotency, the cutting out of stones, ulcers and tumors – truly procedures that in the near future will be seen as barbaric and unscientific.
There is no question that one of the most pernicious practices in vogue today is treating so-called disease with disease and immunizing or vaccinating with the products of disease. Current medical science calls this form of pathological thinking a “vaccination.” When the cause is not known, how is prevention or cure possible except by luck? Producing a mild form of smallpox using vaccine is the same as introducing a poison into a healthy person. It makes no sense. Certainly only pathological thinking can arrive at such conclusions. Vaccine or autogenous remedies (metabolic, dietary, environmental and respiratory acids) are made from the products of disease. The idea that disease can be made to cure itself is an end-product of pathological thinking! If prevention and cure mean producing disease, surely prevention and cure are not desirable. If prevention can be accomplished, then cures will not be needed! It is not disease, it is cause “in all its aspects” that we need to know before we can take steps to prevent or cure “disease.” Cause is constant, ever-present, and always the same. Only effects, and the object on which a cause acts, change. And the change is most inconstant.[3]
To illustrate: a catarrh of the stomach presents first irritation, then inflammation, then ulceration, and finally induration and cancer. Not all cases run true to form. Only a small percentage evolve to ulcer and fewer reach the cancer stage. More toxins exit via acute food poisoning or acute indigestion then by chronic diseases. Most Americans are challenged with the symptomatology of indigestion, which can include acid reflux, diarrhea and/or constipation. The proper way to study disease is to study health and every influence favorable or not favorable to its continuance. This is exactly what I have done and have published numerous peer-reviewed scientific articles on this subject. Our Western system of medicine has been preoccupied with the study of disease, not health. Disease is perverted health. Any influence that lowers energy becomes disease-producing.
Disease cannot be its own cause, neither can it be its own cure and certainly not is own prevention!
My personal discovery of the truth of ALL sickness and disease—that systemic acidosis of the interstitial fluids of the Interestitium is the cause of all so-called diseases—came about slowly, step by step, line upon line, precept upon precept, here a little and there a little. At first, I postulated that yeast and molds must be the general cause of disease. Then I decided that it was not yeast and mold but that the body becoming enervated. But wait a minute, enervation is not a disease; disease must be due to metabolic acids. I reasoned that localized or systemic acidosis in the interstitial fluids of the Interstitium is the true general cause of all disease and must be autogenerated. And if disease is due to autogenerated acids, what is the cause of that auto-generation?
How could I then measure the chemistry, including the pH of an organ that had never been studied and measured quantitatively before? The ability to test and quantify the chemistry, including the pH of the largest organ of the body, the interstitial fluids of the Interstitium was finally published by myself and Dr. Galina Migalko, a scientist and a medical doctor from the Ukraine and now living and working in the USA for over 20 years. Our peer-reviewed article on the chemistry and pH of the arterial blood, the venous blood, the interstitial fluids and the intracellular fluids and their relationship to ALL cancerous conditions was finally published by the International Journal of Complimentary and Alternative Medicine in November of 2015. Our article is entitled, “Alkalizing Nutritional Therapy in the Prevention and Reversal of Any Cancerous Condition,” which finally quantifies ALL of the chemistry, including the pH of all body fluids in a healthy and a sick or cancerous body. [1]

So, what is the answer to the question that if ALL disease is due to autogenerated acids, then what is the cause of that auto-generation?
The answer is found in understanding the nature of matter and how it organizes and disorganizes. I realized that there must be a physical or emotional disturbance to organized matter before it can begin its disorganization. And when matter begins to disorganize, it gives rise to autogenerated acids that can be measured and quantified in the blood and interstitial fluids of the Interstitium. This is true for all matter that is disorganizing or breaking down!
To illustrate, take a physical injury to a joint which is often complicated with the prior symptom of rheumatism. The rheumatism previous to the injury was potentially in the blood and/or interstitial fluids. Just what change had taken place in the matter which, under stress of injury or shock of any kind, would caused a reaction with fever? I could not understand until the “Acid or pH Theory” of the interstitial fluids and blood suggested itself to my mind. After that, the cause of disease unfolded before me in an easy and natural manner. I called this new paradigm for ALL sickness and disease “The Cycle of Imbalance.” You can read about “The Cycle of Imbalance” in my book, “Sick and Tired, Reclaim You Inner Terrain.” You can order this book at: www.phoreveryoung.com.

In a few words, without acidosis of the interstitial fluids, there can be no sickness or disease and there can be NO CANCER! It is also true that without acidosis in the interstitial fluids there can be NO PAIN! Therefore, pain equals acid and acid equals pain. I knew that the waste products of cellular disorganization and metabolism were toxic and that the only reason why we were not poisoned by it was because it was removed from the organism as fast as it was produced.
Then we discovered that the acid was retained in the blood and then interstitial fluids of the Interstitium when there was a checking of elimination. Then, the cause of the checking had to be determined. In time, I thought out the cause of all sickness and disease. I knew that when we had normal energy, organic functioning was normal. Then came the discovery that enervation caused a checking of elimination.
Eureka! The cause of ALL sickness and disease is NOW found! Enervation checks elimination of the waste-products — ACIDS — of cellular disorganization and metabolism. Retention of metabolic ACIDS is the first and the only cause of sickness and disease! [4 through 52]
One of the first things to do to get rid of any so-called disease is to get rid of all the acid, for it is this state of the blood and tissues that makes disease possible. Infection, drugs and food poisoning may kill, but if they do not, they will be short-lived in a subject that is free from enervation and the acidic waste that causes sickness and disease. Conversely, the poisoning will linger in the system until the acid is overcome. Then and only then will elimination remove all traces of the outfection from the cells.
Syphilitic outfection is pronouncedly an acidic subject thrown into great virulency by poor nutrition, lifestyle and conventional treatment. The same is true with HIV/AIDS. The so-called infection is the least offender of the trio. Add fear (false evidence appearing real) and wrong eating and we have a formidable symptom complex that serves to justify all that professional syphilomaniacs say and write about the disease. Remove acidosis, drugging, fear, and vile eating, and there is little left. What is left can be easily thrown out of the body by Nature! Scientific research is being carried on vigorously in an attempt to find the cause of disease. The conception of disease is that the cause is individual. Here is where investigators meet their Waterloo. All of the so-called diseases are increasing symptom complexes due to repeated crises of acidosis of the interstitial fluids of the Interstitium. They have no independent existence! As soon as acidity is controlled, the symptoms disappear unless an organ has been forced by innumerable crises to degenerate. Even organic change, when the organ is not destroyed, will come back by correcting the lifesytle and getting rid of the true cause—the crisis of systemic acidosis discovered by myself and Dr. Galina Migalko, MD!

All symptoms of all so-called diseases have one origin. All diseases are ONE! Unity in all things is Nature’s plan. Polytheism is gone, and everything pertaining to it and coming out of it must go. So there is only one sickness, one disease, and NOW one treatment. The one sickness and disease is the over-acidification of the interstitial fluids of the Interstitium and then the blood due to an inverted way of living, eating, and thinking. The one treatment is to alkalize and energize with the pH Miracle Lifestyle and Dietary Plan. You can learn more about this program on our website or in our books, The pH Miracle, The pH Miracle for Diabetes, The pH Miracle for Weight Loss, The pH Miracle for Cancer, The Cancer Solution, Reverse Cancer NOW1, Back to the House of Health I and II and Sick and Tired which you can also purchase through Amazon.com or Barnes and Noble.

The complete program is a 12 week program that includes the foods outlined in the foundational section of the book, “Back to the House of Health.” You start off the program with a 10 to 14 day liquid feast. You can eat as much and as often as you like as long as the food is green and purred. The soups found in the pH Miracle books such as the Broccoli Soup, Aspar/Zinc Soup, The Healing Soup and the Popeye Soup with lots of avocados are excellent to eat during the liquid feast. You also need to begin taking the nutritional supplements while drinking at least 4 to 6 liters of iJuice Super Greens a day. Start out gradually drinking 1 liter of Greens per day and then work up to 2, then 3, then 4, until you are drinking 6 liters a day.(www.phmiracleproducts.com)

When you take the nutritional supplements, take 5 drops 6 times a day of the liquid colloids under the tongue, (except the pH drops which are taken in purified water and NEVER taken under the tongue) away from meals, or taking 1 capsule 6 times a day of the capsule products with meals. I would suggest taking 4 capsules every 4 waking hours of the bowel cleansing formula. The bowel cleansing product helps to keep things moving through normal elimination.
After you complete the 10 to 14 day liquid feast, you can then begin introducing some solid food but it still needs to be as green as possible. I would suggest not only the vegetable soups, but steam fry vegetables and lots of green salads. Make sure you use only lemon or lime and good oils on your salads for the dressing. Another tip is to include liberal amounts of flax and olive oil in or with your soups and salads. I suggest a minimum of 5 to 6 tablespoons of good oils each day.

In conclusion, the medical world has been looking for a remedy to cure disease, notwithstanding the obvious fact that nature needs no remedy. She needs only an opportunity to exercise her own prerogative of self-healing.
Cures! There are NO cures! The subconscious builds health or disease according to OUR ORDER. If we send impulses of irritation, discontent, unhappiness, complaining, hate, envy, selfishness, greed, lust, and the biggest one of all pride, the subconscious builds us in the image of OUR ORDER!
The truth is that we need no doctor. We need to empower ourselves to effect a reconciliation between our subconscious creator and ourselves. What we need is to learn self-control, respect, poise, and relaxation! And when these impulses are sent over the sympathetic nerves to our subconscious creator, we will begin to receive images of a more ideal man or woman, until an approach to “Perfection is Attained.”
Sickness and disease, including the symptoms of heart disease, cancer, tumors, AIDS, diabetes, MS, lupus, HIV/AIDS, depression, hyperthyroidism, Wilson’s Syndrome, fybromyalgia, pain in every joint and muscle, chronic fatigue syndrome, muscle cramps, allergies (food), asthma, bronchitis, frequent colds, candida, hypoglycemia, allergic reaction to any chemical, chronic fatiguing, food cravings, indigestion, inflamed joints, insomnia, mood swings, gas, bloating, diverticulitis, irritable bowel, pneumonia, ulcers, stomach and bowel cramps and even memory loss is the culmination of years of abuse of nutrition and years of acids from faulty elimination by forcing the bowels to move. We don’t GET sick and tired we DO sick and tired!
The most powerful way to eliminate acids in the interstitial fluids of the Interstitium and the blood is the pH Miracle Lifestyle and Dietary Plan.

You are the builder of tomorrow, and you need not pay a fortune-teller, a doctor, a lawyer, a preacher, or a banker to tell you what will happen to you tomorrow. Nothing will happen. The inevitable will come. You will inherit the fruits of today’s sowing. I hope you find these thoughts and suggestions helpful when dealing with any symptomatology, whether physical, emotional or spiritual.
To learn more about the work, research and findings of Robert O Young CPT, MSc, DSc, PhD, Naturopathic Practitioner go to: www.drrobertyoung.com

To learn more about testing the chemistry including the pH of the blood and the interstitial fluids go to: www.universalmedicalimaging.com

References
[1] Young RO, Migalko G (2015) Alkalizing Nutritional Therapy in the Prevention and Reversal of any Cancerous Condition. Int J Complement Alt Med 2(1): 00046. DOI: 10.15406/ijcam.2015.02.00046
[2] Young, RO, Metabolic and Dietary Acids are the Fuel that Lights the Fuse that Ignites Inflammation that Leads to Cancer!. Int J Complement Alt Med 3(6): 00094. DOI: 10.15406/ijcam.2016.03.00094
[3] Young RO (2016) Second Thoughts about Viruses, Vaccines, and the HIV/AIDS Hypothesis – Part 1. Int J Vaccines Vaccin 2(3): 00032. DOI: 10.15406/ijvv.2016.02.0003
[4] Ströhle A, Hahn A, Sebastian A. Estimation of the diet-dependent net acid load in 229 worldwide historically studied hunter-gatherer societies. American Journal of Clinical Nutrition. 2010;91(2):406–412.[PubMed]
[5] Sebastian A, Frassetto LA, Sellmeyer DE, Merriam RL, Morris RC., Jr. Estimation of the net acid load of the diet of ancestral preagricultural Homo sapiens and their hominid ancestors. American Journal of Clinical Nutrition. 2002;76(6):1308–1316. [PubMed]
[6] Frassetto L, Morris, Jr. R.C. RC, Jr., Sellmeyer DE, Todd K, Sebastian A. Diet, evolution and aging—the pathophysiologic effects of the post-agricultural inversion of the potassium-to-sodium and base-to-chloride ratios in the human diet. European Journal of Nutrition. 2001;40(5):200–213. [PubMed]
[7] Konner M, Boyd Eaton S. Paleolithic nutrition: twenty-five years later. Nutrition in Clinical Practice. 2010;25(6):594–602. [PubMed]
[8] Lindeman RD, Goldman R. Anatomic and physiologic age changes in the kidney. Experimental Gerontology. 1986;21(4-5):379–406. [PubMed]
[9] Reddy ST, Wang CY, Sakhaee K, Brinkley L, Pak CY. Effect of low-carbohydrate high-protein diets on acid-base balance, stone-forming propensity, and calcium metabolism. American Journal of Kidney Diseases. 2002;40(2):265–274. [PubMed]
[10] Malov YS, Kulikov AN. Bicarbonate deficiency and duodenal ulcer. Terapevticheskii Arkhiv. 1998;70(2):28–32. [PubMed]
[11] Ohman H, Vahlquist A. In vivo studies concerning a pH gradient in human stratum corneum and upper epidermis. Acta Dermato-Venereologica. 1994;74(5):375–379. [PubMed]
[12] Ferris DG, Francis SL, Dickman ED, Miler-Miles K, Waller JL, McClendon N. Variability of vaginal pH determination by patients and clinicians. Journal of the American Board of Family Medicine. 2006;19(4):368–373. [PubMed]
[13] Remer T, Manz F. Estimation of the renal net acid excretion by adults consuming diets containing variable amounts of protein. American Journal of Clinical Nutrition. 1994;59(6):1356–1361. [PubMed]
[14] Remer T. Influence of diet on acid-base balance. Seminars in Dialysis. 2000;13(4):221–226. [PubMed]
[15] Fenton TR, Eliasziw M, Tough SC, Lyon AW, Brown JP, Hanley DA. Low urine pH and acid excretion do not predict bone fractures or the loss of bone mineral density: a prospective cohort study. BMC Musculoskeletal Disorders. 2010;11, article 88 [PMC free article] [PubMed]
[16] Boelsma E, van de Vijver LPL, Goldbohm RA, Klöpping-Ketelaars IAA, Hendriks HFJ, Roza L. Human skin condition and its associations with nutrient concentrations in serum and diet. American Journal of Clinical Nutrition. 2003;77(2):348–355. [PubMed]
[17] Ince BA, Anderson EJ, Neer RM. Lowering dietary protein to U.S. recommended dietary allowance levels reduces urinary calcium excretion and bone resorption in young women. Journal of Clinical Endocrinology and Metabolism. 2004;89(8):3801–3807. [PubMed]
[18] Boron WF. Regulation of intracellular pH. Advances in Physiology Education. 2004;28:160–179.[PubMed]
[19] Remer T, Manz F. Potential renal acid load of foods and its influence on urine pH. Journal of the American Dietetic Association. 1995;95(7):791–797. [PubMed]
[20] Fenton TR, Eliasziw M, Lyon AW, Tough SC, Hanley DA. Meta-analysis of the quantity of calcium excretion associated with the net acid excretion of the modern diet under the acid-ash diet hypothesis. American Journal of Clinical Nutrition. 2008;88(4):1159–1166. [PubMed]
[21] Sebastian A, Morris RC., Jr. Improved mineral balance and skeletal metabolism in postmenopausal women treated with potassium bicarbonate. New England Journal of Medicine. 1994;331(4):p. 279.[PubMed]
[22] Dawson-Hughes B, Harris SS, Palermo NJ, Castaneda-Sceppa C, Rasmussen HM, Dallal GE. Treatment with potassium bicarbonate lowers calcium excretion and bone resorption in older men and women. Journal of Clinical Endocrinology and Metabolism. 2009;94(1):96–102. [PMC free article][PubMed]
[23] Heaney RP, Dowell MS, Hale CA, Bendich A. Calcium absorption varies within the reference range for serum 25-hydroxyvitamin D. Journal of the American College of Nutrition. 2003;22(2):142–146.[PubMed]
[24] Schwalfenberg GK, Genuis SJ, Hiltz MN. Addressing vitamin D deficiency in Canada: a public health innovation whose time has come. Public Health. 2010;124(6):350–359. [PubMed]
[25] Lu KC, Lin SH, Yu FC, Chyr SH, Shieh SD. Influence of metabolic acidosis on serum 1,25(OH)2D3 levels in chronic renal failure. Mineral and Electrolyte Metabolism. 1995;21(6):398–402. [PubMed]
[26] Fenton TR, Lyon AW, Eliasziw M, Tough SC, Hanley DA. Phosphate decreases urine calcium and increases calcium balance: a meta-analysis of the osteoporosis acid-ash diet hypothesis. Nutrition Journal. 2009;8, article 41 [PMC free article] [PubMed]
[27] Hulley SB, Vogel JM, Donaldson CL, Bayers JH, Friedman RJ, Rosen SN. The effect of supplemental oral phosphate on the bone mineral changes during prolonged bed rest. Journal of Clinical Investigation. 1971;50(12):2506–2518. [PMC free article] [PubMed]
[28] Fenton TR, Lyon AW, Eliasziw M, Tough SC, Hanley DA. Meta-analysis of the effect of the acid-ash hypothesis of osteoporosis on calcium balance. Journal of Bone and Mineral Research. 2009;24(11):1835–1840. [PubMed]
[29] Supplee JD, Duncan GE, Bruemmer B, Goldberg J, Wen Y, Henderson JA. Soda intake and osteoporosis risk in postmenopausal American-Indian women. Public Health Nutrition. 2011:1–7.[PMC free article] [PubMed]
[30] Fenton TR, Tough SC, Lyon AW, Eliasziw M, Hanley DA. Causal assessment of dietary acid load and bone disease: a systematic review & meta-analysis applying Hill’s epidemiologic criteria for causality. Nutrition Journal. 2011;10(1, article 41) [PMC free article] [PubMed]
[31] Frassetto LA, Morris RC, Jr., Sebastian A. Dietary sodium chloride intake independently predicts the degree of hyperchloremic metabolic acidosis in healthy humans consuming a net acid-producing diet. American Journal of Physiology—Renal Physiology. 2007;293(2):F521–F525. [PubMed]
[32] Frings-Meuthen P, Buehlmeier J, Baecker N, et al. High sodium chloride intake exacerbates immobilization-induced bone resorption and protein losses. Journal of Applied Physiology. 2011;111(2):537–542. [PubMed]
[33] Cappuccio FP, Meilahn E, Zmuda JM, Cauley JA. High blood pressure and bone-mineral loss in elderly white women: a prospective study. Lancet. 1999;354(9183):971–975. [PubMed]
[34] Devine A, Criddle RA, Dick IM, Kerr DA, Prince RL. A longitudinal study of the effect of sodium and calcium intakes on regional bone density in postmenopausal women. American Journal of Clinical Nutrition. 1995;62(4):740–745. [PubMed]
[35] Morris RC, Jr., Schmidlin O, Frassetto LA, Sebastian A. Relationship and interaction between sodium and potassium. Journal of the American College of Nutrition. 2006;25(3):262S–270S. [PubMed]
[36] Barzel US, Massey LK. Excess dietary protein may can adversely affect bone. Journal of Nutrition. 1998;128(6):1051–1053. [PubMed]
[37] Heaney RP, Layman DK. Amount and type of protein influences bone health. American Journal of Clinical Nutrition. 2008;87(5):156S–157S. [PubMed]
[38] Dawson-Hughes B, Harris SS, Ceglia L. Alkaline diets favor lean tissue mass in older adults. American Journal of Clinical Nutrition. 2008;87(3):662–665. [PMC free article] [PubMed]
[39] Garibotto G, Russo R, Sofia A, et al. Muscle protein turnover in chronic renal failure patients with metabolic acidosis or normal acid-base balance. Mineral and Electrolyte Metabolism. 1996;22(1–3):58–61.[PubMed]
[40] Caso G, Garlick PJ. Control of muscle protein kinetics by acid-base balance. Current Opinion in Clinical Nutrition and Metabolic Care. 2005;8(1):73–76. [PubMed]
[41] Webster MJ, Webster MN, Crawford RE, Gladden LB. Effect of sodium bicarbonate ingestion on exhaustive resistance exercise performance. Medicine and Science in Sports and Exercise. 1993;25(8):960–965. [PubMed]
[42] McSherry E, Morris RC., Jr. Attainment and maintenance of normal stature with alkali therapy in infants and children with classic renal tubular acidosis. Journal of Clinical Investigation. 1978;61(2):509–527. [PMC free article] [PubMed]
[43] Frassetto L, Morris RC, Jr., Sebastian A. Potassium bicarbonate reduces urinary nitrogen excretion in postmenopausal women. Journal of Clinical Endocrinology and Metabolism. 1997;82(1):254–259.[PubMed]
[44] Wass JAH, Reddy R. Growth hormone and memory. Journal of Endocrinology. 2010;207(2):125–126.[PubMed]
[45] Frassetto L, Morris RC, Jr., Sebastian A. Long-term persistence of the urine calcium-lowering effect of potassium bicarbonate in postmenopausal women. Journal of Clinical Endocrinology and Metabolism. 2005;90(2):831–834. [PubMed]
[46] Vormann J, Worlitschek M, Goedecke T, Silver B. Supplementation with alkaline minerals reduces symptoms in patients with chronic low back pain. Journal of Trace Elements in Medicine and Biology. 2001;15(2-3):179–183. [PubMed]
[47] Zofková I, Kancheva RL. The relationship between magnesium and calciotropic hormones. Magnesium Research. 1995;8(1):77–84. [PubMed]
[48] Schwalfenberg G. Improvement of chronic back pain or failed back surgery with vitamin D repletion: a case series. Journal of the American Board of Family Medicine. 2009;22(1):69–74. [PubMed]
[49] Groos E, Walker L, Masters JR. Intravesical chemotherapy. Studies on the relationship between pH and cytotoxicity. Cancer. 1986;58(6):1199–1203. [PubMed]
[50] Smith SR, Martin PA, Edwards RHT. Tumour pH and response to chemotherapy: an in vivo 31P magnetic resonance spectroscopy study in non-Hodgkin’s lymphoma. British Journal of Radiology. 1991;64(766):923–928. [PubMed]
[51] Raghunand N, Gillies RJ. pH and chemotherapy. Novartis Foundation Symposium. 2001;240:199–211.[PubMed]
[52] Raghunand N, He X, Van Sluis R, et al. Enhancement of chemotherapy by manipulation of tumour pH. British Journal of Cancer. 1999;80(7):1005–1011. [PMC free article] [PubMed]