Low Levels of Sodium Bicarbonate in Blood and Interstitial fluids Increases the Risk of Death!
Lower than normal levels of sodium and potassium bicarbonate in the blood, interstitial fluids of the Interstitium and the intracellular fluids increases the risk of death by 24%.
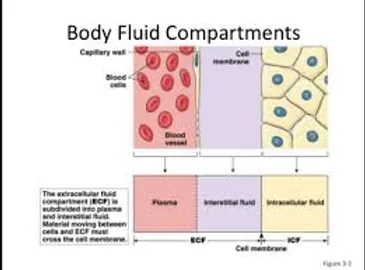
Research published in the Clinical Journal of the American Society of Nephrology found that having sufficient levels of sodium bicarbonate, or bicarbonate in your body fluids can reduce your chances of an early death! Maintaining bicarbonates greater than 24 mEq/L of the blood and interstitial fluids may increase the quality of life while increasing life expectancy 20 years or more according to the research and findings of Dr. Robert O. Young[1]
The study examined data compiled in the Health, Aging and Body Composition Study for 2,287 participants.
Participants were healthy adults who, at the onset of the study, were between the ages of 70 and 79, and were followed for approximately 10 years. Survival data were gathered through February, 2014.
Raphael and colleagues found that low levels of sodium bicarbonate can be linked to an increased risk for premature death by 24 percent. Sodium bicarbonate is the main buffer for metabolic, dietary, environmental and respiratory acidic waste. Managing and maintaining the delicate pH balance of the intravascular and interstitial fluids of the Interstitium with sodium and potassium bicarbonate may extend life expectancy by up to 20 years or more!
“What we found was that healthy older people with low levels of sodium bicarbonate had a higher risk of death,” Raphael said. The study’s findings can assist clinicians in better assessing a patient’s risk of premature death by analyzing their blood and interstitial fluid bicarbonate concentrations more closely and by taking the pH Miracle pHour Salts!

To order go to: https://www.phmiracleproducts.com/…/ph…/products/phour-salts
Abstract
Background and objectives Low serum bicarbonate associates with mortality in CKD. This study investigated the associations of bicarbonate and acid-base status with mortality in healthy older individuals.
Design, setting, participants, & measurements
We analyzed data from the Health, Aging, and Body Composition Study, a prospective study of well functioning black and white adults ages 70–79 years old from 1997. Participants with arterialized venous blood gas measurements (n=2287) were grouped into <23.0 mEq/L (low), 23.0–27.9 mEq/L (reference group), and ≥28.0 mEq/L (high) bicarbonate categories and according to acid-base status. Survival data were collected through February of 2014. Mortality hazard ratios (HRs; 95% confidence intervals [95% CIs]) in the low and high bicarbonate groups compared with the reference group were determined using Cox models adjusted for demographics, eGFR, albuminuria, chronic obstructive pulmonary disease, smoking, and systemic pH. Similarly adjusted Cox models were performed according to acid-base status.
Results
The mean age was 76 years, 51% were women, and 38% were black. Mean pH was 7.41, mean bicarbonate was 25.1 mEq/L, 11% had low bicarbonate, and 10% had high bicarbonate. Mean eGFR was 82.1 ml/min per 1.73 m2, and 12% had CKD. Over a mean follow-up of 10.3 years, 1326 (58%) participants died. Compared with the reference group, the mortality HRs were 1.24 (95% CI, 1.02 to 1.49) in the low bicarbonate and 1.03 (95% CI, 0.84 to 1.26) in the high bicarbonate categories. Compared with the normal acid-base group, the mortality HRs were 1.17 (95% CI, 0.94 to 1.47) for metabolic acidosis, 1.21 (95% CI, 1.01 to 1.46) for respiratory alkalosis, and 1.35 (95% CI, 1.08 to 1.69) for metabolic alkalosis categories. Respiratory acidosis did not associate with mortality.
Conclusions
In generally healthy older individuals, low serum bicarbonate was associated with higher mortality..
What does this mean for me?
The answer is simple: living longer and living better!
How do you get more alkalinity in the form of sodium and potassium bicarbonate?
Surprisingly, the answer has everything to do with increasing your pH or alkalinity with sodium and potassium bicarbonate called pHour salts. In addition, you will want to increase your urine pH levels up to 7.8 to 8.4 by getting more sodium and potassium bicarbonate in your diet by eating more fruit and vegetables.

Alkaline Fruit and vegetables high in sodium and potassium bicarbonate will have a negative potential renal acid load (PRAL) score. This represents the amount of acid produced by the kidneys after metabolism. The higher the negative, the more sodium, potassium and bicarbonate they will provide, potentially reducing your risk of premature death, according to the study. Avocados, cucumbers, spinach, celery, grasses, green peppers, tomatoes, garlic, onions, broccoli, lemons, limes and even alkaline water at a pH of 9.5 to 11 are a few sources that will boost your sodium, potassium and bicarbonate levels. [See lists of alkaline foods to eat freely and acidic foods to eliminate]


References
[1] Young RO, Migalko G (2015) Alkalizing Nutritional Therapy in the Prevention and Reversal of any Cancerous Condition. Int J Complement Alt Med 2(1): 00046. DOI:10.15406/ijcam.2015.02.00046
[2] Dobre M, Yang W, Chen J, Drawz P, Hamm LL, Horwitz E, Hostetter T, Jaar B, Lora CM, Nessel L, Ojo A, Scialla J, Steigerwalt S, Teal V, Wolf M, Rahman M, CRIC Investigators: Association of serum bicarbonate with risk of renal and cardiovascular outcomes in CKD: A report from the Chronic Renal Insufficiency Cohort (CRIC) study. Am J Kidney Dis 62: 670–678, 2013pmid:23489677CrossRefPubMedGoogle Scholar
[3] Kovesdy CP, Anderson JE, Kalantar-Zadeh K: Association of serum bicarbonate levels with mortality in patients with non-dialysis-dependent CKD. Nephrol Dial Transplant 24: 1232–1237, 2009pmid:19015169Abstract/FREE Full TextGoogle Scholar
[4] Navaneethan SD, Schold JD, Arrigain S, Jolly SE, Wehbe E, Raina R, Simon JF, Srinivas TR, Jain A, Schreiber MJ Jr.., Nally JV Jr..: Serum bicarbonate and mortality in stage 3 and stage 4 chronic kidney disease. Clin J Am Soc Nephrol 6: 2395–2402, 2011pmid:21885787Abstract/FREE Full TextGoogle Scholar
[5] Raphael KL, Wei G, Baird BC, Greene T, Beddhu S: Higher serum bicarbonate levels within the normal range are associated with better survival and renal outcomes in African Americans. Kidney Int 79: 356–362, 2011pmid:20962743CrossRefPubMedGoogle Scholar
[6] ↵Driver TH, Shlipak MG, Katz R, Goldenstein L, Sarnak MJ, Hoofnagle AN, Siscovick DS, Kestenbaum B, de Boer IH, Ix JH: Low serum bicarbonate and kidney function decline: The Multi-Ethnic Study of Atherosclerosis (MESA). Am J Kidney Dis 64: 534–541, 2014pmid:24953891CrossRefPubMedGoogle Scholar
[7] ↵Goldenstein L, Driver TH, Fried LF, Rifkin DE, Patel KV, Yenchek RH, Harris TB, Kritchevsky SB, Newman AB, Sarnak MJ, Shlipak MG, Ix JH, Health ABC Study Investigators: Serum bicarbonate concentrations and kidney disease progression in community-living elders: The Health, Aging, and Body Composition (Health ABC) Study. Am J Kidney Dis 64: 542–549, 2014pmid:24953890CrossRefPubMedGoogle Scholar
[8] ↵Shah SN, Abramowitz M, Hostetter TH, Melamed ML: Serum bicarbonate levels and the progression of kidney disease: A cohort study. Am J Kidney Dis 54: 270–277, 2009pmid:19394734CrossRefPubMedGoogle Scholar
[9] ↵Raphael KL, Zhang Y, Wei G, Greene T, Cheung AK, Beddhu S: Serum bicarbonate and mortality in adults in NHANES III. Nephrol Dial Transplant 28: 1207–1213, 2013pmid:23348878Abstract/FREE Full TextGoogle Scholar
[10] ↵Inker LA, Schmid CH, Tighiouart H, Eckfeldt JH, Feldman HI, Greene T, Kusek JW, Manzi J, Van Lente F, Zhang YL, Coresh J, Levey AS, CKD-EPI Investigators: Estimating glomerular filtration rate from serum creatinine and cystatin C. N Engl J Med 367: 20–29, 2012pmid:22762315CrossRefPubMedGoogle Scholar
[11] ↵Bibbins-Domingo K, Chertow GM, Fried LF, Odden MC, Newman AB, Kritchevsky SB, Harris TB, Satterfield S, Cummings SR, Shlipak MG: Renal function and heart failure risk in older black and white individuals: The Health, Aging, and Body Composition Study. Arch Intern Med 166: 1396–1402, 2006pmid:16832005CrossRefPubMedGoogle Scholar
[12] ↵O’Donovan A, Pantell MS, Puterman E, Dhabhar FS, Blackburn EH, Yaffe K, Cawthon RM, Opresko PL, Hsueh WC, Satterfield S, Newman AB, Ayonayon HN, Rubin SM, Harris TB, Epel ES, Health Aging and Body Composition Study: Cumulative inflammatory load is associated with short leukocyte telomere length in the Health, Aging and Body Composition Study. PLoS One 6: e19687, 2011pmid:21602933CrossRefPubMedGoogle Scholar
[13] ↵Visser M, Fuerst T, Lang T, Salamone L, Harris TB: Validity of fan-beam dual-energy X-ray absorptiometry for measuring fat-free mass and leg muscle mass. Health, Aging, and Body Composition Study–Dual-Energy X-ray Absorptiometry and Body Composition Working Group. J Appl Physiol (1985) 87: 1513–1520, 1999
[14] ↵Fuller NJ, Laskey MA, Elia M: Assessment of the composition of major body regions by dual-energy X-ray absorptiometry (DEXA), with special reference to limb muscle mass. Clin Physiol 12: 253–266, 1992pmid:1606809CrossRefPubMedGoogle Scholar
[15] ↵Waterer GW, Wan JY, Kritchevsky SB, Wunderink RG, Satterfield S, Bauer DC, Newman AB, Taaffe DR, Jensen RL, Crapo RO, Health ABC Study: Airflow limitation is underrecognized in well-functioning older people. J Am Geriatr Soc 49: 1032–1038, 2001pmid:11555063CrossRefPubMedGoogle Scholar
[16] ↵Raphael KL, Zhang Y, Ying J, Greene T: Prevalence of and risk factors for reduced serum bicarbonate in chronic kidney disease. Nephrology (Carlton) 19: 648–654, 2014
[17] ↵Gennari FJ, Hood VL, Greene T, Wang X, Levey AS: Effect of dietary protein intake on serum total CO2 concentration in chronic kidney disease: Modification of Diet in Renal Disease study findings. Clin J Am Soc Nephrol 1: 52–57, 2006pmid:17699190Abstract/FREE Full TextGoogle Scholar
[18] ↵Bailey JL, Wang X, England BK, Price SR, Ding X, Mitch WE: The acidosis of chronic renal failure activates muscle proteolysis in rats by augmenting transcription of genes encoding proteins of the ATP-dependent ubiquitin-proteasome pathway. J Clin Invest 97: 1447–1453, 1996pmid:8617877CrossRefPubMedGoogle Scholar
[19] ↵Farwell WR, Taylor EN: Serum anion gap, bicarbonate and biomarkers of inflammation in healthy individuals in a national survey. CMAJ 182: 137–141, 2010pmid:20008503Abstract/FREE Full TextGoogle Scholar
[20] ↵Nath KA, Hostetter MK, Hostetter TH: Pathophysiology of chronic tubulo-interstitial disease in rats. Interactions of dietary acid load, ammonia, and complement component C3. J Clin Invest 76: 667–675, 1985pmid:2993363CrossRefPubMedGoogle Scholar
[20] Wesson DE, Dolson GM: Endothelin-1 increases rat distal tubule acidification in vivo. Am J Physiol 273: F586–F594, 1997pmid:9362336PubMedGoogle Scholar
[21] ↵Wesson DE, Simoni J: Increased tissue acid mediates a progressive decline in the glomerular filtration rate of animals with reduced nephron mass. Kidney Int 75: 929–935, 2009pmid:19190678CrossRefPubMedGoogle Scholar
[22] ↵Bushinsky DA, Chabala JM, Gavrilov KL, Levi-Setti R: Effects of in vivo metabolic acidosis on midcortical bone ion composition. Am J Physiol 277: F813–F819, 1999pmid:10564247PubMedGoogle Scholar
[23] ↵May RC, Kelly RA, Mitch WE: Mechanisms for defects in muscle protein metabolism in rats with chronic uremia. Influence of metabolic acidosis. J Clin Invest 79: 1099–1103, 1987pmid:3549778CrossRefPubMedGoogle Scholar
[24] ↵Bellocq A, Suberville S, Philippe C, Bertrand F, Perez J, Fouqueray B, Cherqui G, Baud L: Low environmental pH is responsible for the induction of nitric-oxide synthase in macrophages. Evidence for involvement of nuclear factor-kappaB activation. J Biol Chem 273: 5086–5092, 1998pmid:9478960Abstract/FREE Full TextGoogle Scholar
[25] ↵Ng HY, Chen HC, Tsai YC, Yang YK, Lee CT: Activation of intrarenal renin-angiotensin system during metabolic acidosis. Am J Nephrol 34: 55–63, 2011pmid:21659740CrossRefPubMedGoogle Scholar
[26] ↵Wood CE, Isa A: Intravenous acid infusion stimulates ACTH secretion in sheep. Am J Physiol 260: E154–E161, 1991pmid:1846273PubMedGoogle Scholar
[27] ↵Ordóñez FA, Santos F, Martínez V, García E, Fernández P, Rodríguez J, Fernández M, Alvarez J, Ferrando S: Resistance to growth hormone and insulin-like growth factor-I in acidotic rats. Pediatr Nephrol 14: 720–725, 2000pmid:10955915CrossRefPubMedGoogle Scholar
[28] ↵de Brito-Ashurst I, Varagunam M, Raftery MJ, Yaqoob MM: Bicarbonate supplementation slows progression of CKD and improves nutritional status. J Am Soc Nephrol 20: 2075–2084, 2009pmid:19608703Abstract/FREE Full TextGoogle Scholar
[29] Litzow JR, Lemann J Jr.., Lennon EJ: The effect of treatment of acidosis on calcium balance in patients with chronic azotemic renal disease. J Clin Invest 46: 280–286, 1967pmid:6018764CrossRefPubMedGoogle Scholar
[30] Löfberg E, Gutierrez A, Anderstam B, Wernerman J, Bergström J, Price SR, Mitch WE, Alvestrand A: Effect of bicarbonate on muscle protein in patients receiving hemodialysis. Am J Kidney Dis 48: 419–429, 2006pmid:16931215CrossRefPubMedGoogle Scholar
[31] ↵Mathur RP, Dash SC, Gupta N, Prakash S, Saxena S, Bhowmik D: Effects of correction of metabolic acidosis on blood urea and bone metabolism in patients with mild to moderate chronic kidney disease: A prospective randomized single blind controlled trial. Ren Fail 28: 1–5, 2006pmid:16526312CrossRefPubMedGoogle Scholar
[32] ↵Koenig J, Loerbroks A, Jarczok MN, Fischer JE, Thayer JF: Chronic pain and heart rate variability in a cross-sectional occupational sample: Evidence for impaired vagal control [published online ahead of print April 28, 2015]. Clin J Painpmid:25924095PubMedGoogle Scholar
[33] ↵Dekker JM, Crow RS, Folsom AR, Hannan PJ, Liao D, Swenne CA, Schouten EG: Low heart rate variability in a 2-minute rhythm strip predicts risk of coronary heart disease and mortality from several causes: The ARIC Study. Atherosclerosis Risk In Communities. Circulation 102: 1239–1244, 2000pmid:10982537Abstract/FREE Full TextGoogle Scholar
[34] ↵Butnoriene J, Bunevicius A, Saudargiene A, Nemeroff CB, Norkus A, Ciceniene V, Bunevicius R: Metabolic syndrome, major depression, generalized anxiety disorder, and ten-year all-cause and cardiovascular mortality in middle aged and elderly patients. Int J Cardiol 190: 360–366, 2015pmid:25939128CrossRefPubMedGoogle Scholar
[35] ↵Anderson LE, Henrich WL: Alkalemia-associated morbidity and mortality in medical and surgical patients. South Med J 80: 729–733, 1987pmid:3589765CrossRefPubMedGoogle Scholar
[36] ↵Bellingham AJ, Detter JC, Lenfant C: Regulatory mechanisms of hemoglobin oxygen affinity in acidosis and alkalosis. J Clin Invest 50: 700–706, 1971pmid:5545127CrossRefPubMedGoogle Scholar
[37] ↵de Solis AJ, González-Pacheco FR, Deudero JJ, Neria F, Albalate M, Petkov V, Susanibar L, Fernandez-Sanchez R, Calabia O, Ortiz A, Caramelo C: Alkalinization potentiates vascular calcium deposition in an uremic milieu. J Nephrol 22: 647–653, 2009pmid:19809998PubMedGoogle Scholar
[38] ↵Gaggl M, Cejka D, Plischke M, Heinze G, Fraunschiel M, Schmidt A, Hörl WH, Sunder-Plassmann G: Effect of oral sodium bicarbonate supplementation on progression of chronic kidney disease in patients with chronic metabolic acidosis: Study protocol for a randomized controlled trial (SoBic-Study). Trials 14: 196, 2013pmid:23826760CrossRefPubMedGoogle Scholar
[39] Phisitkul S, Khanna A, Simoni J, Broglio K, Sheather S, Rajab MH, Wesson DE: Amelioration of metabolic acidosis in patients with low GFR reduced kidney endothelin production and kidney injury, and better preserved GFR. Kidney Int 77: 617–623, 2010pmid:20072112CrossRefPubMedGoogle Scholar
[40] ↵Witham MD, Band MM, Littleford RC, Avenell A, Soiza RL, McMurdo ME, Sumukadas D, Ogston SA, Lamb EJ, Hampson G, McNamee P, BiCARB Study Group: Does oral sodium bicarbonate therapy improve function and quality of life in older patients with chronic kidney disease and low-grade acidosis (the BiCARB trial)? Study protocol for a randomized controlled trial. Trials 16: 326, 2015pmid:26231610CrossRefPubMedGoogle Scholar
[41] ↵Buehlmeier J, Frings-Meuthen P, Remer T, Maser-Gluth C, Stehle P, Biolo G, Heer M: Alkaline salts to counteract bone resorption and protein wasting induced by high salt intake: Results of a randomized controlled trial. J Clin Endocrinol Metab 97: 4789–4797, 2012pmid:23027921CrossRefPubMedGoogle Scholar
[42] He FJ, Marciniak M, Carney C, Markandu ND, Anand V, Fraser WD, Dalton RN, Kaski JC, MacGregor GA: Effects of potassium chloride and potassium bicarbonate on endothelial function, cardiovascular risk factors, and bone turnover in mild hypertensives. Hypertension 55: 681–688, 2010pmid:20083724Abstract/FREE Full TextGoogle Scholar
[43] Ceglia L, Harris SS, Abrams SA, Rasmussen HM, Dallal GE, Dawson-Hughes B: Potassium bicarbonate attenuates the urinary nitrogen excretion that accompanies an increase in dietary protein and may promote calcium absorption. J Clin Endocrinol Metab 94: 645–653, 2009pmid:19050051CrossRefPubMedGoogle Scholar
[44] ↵Frassetto L, Morris RC Jr.., Sebastian A: Long-term persistence of the urine calcium-lowering effect of potassium bicarbonate in postmenopausal women. J Clin Endocrinol Metab 90: 831–834, 2005pmid:15572425CrossRefPubMedGoogle Scholar
[45] ↵Kirschbaum B: Spurious metabolic acidosis in hemodialysis patients. Am J Kidney Dis 35: 1068–1071, 2000pmid:10845818CrossRefPubMedGoogle Scholar